Urethral Stricture Disease
When scar tissue forms along the urethra - the tube through which we urinate - it is called a urethral stricture. This results in narrowing of the channel and can have very harmful effects. Some of the more serious problems we can see are kidney failure, urinary tract infections, and complete urinary retention (an inability to urinate at all). Earlier problems that develop include a weakening of the urinary stream, urinary frequency, urgency, double voiding, spraying of the stream, and painful urination. These symptoms have significant overlap with BPH (enlarged prostate). Making an diagnosis is crucial to determining appropriate treatment. For example, there are no medication options for stricture disease since this is a fixed obstruction. Sometimes an enlarged prostate and urethral stricture can both exist and it is not uncommon to need to treat both.
When a stricture is first identified, it is commonly treated endoscopically (through a camera scope). We can use an assortment of devices such as a laser, cautery, balloon, etc. The recurrence rate for strictures is quite high. We now have good evidence to first try an endoscopic repair but if that fails to then consider moving on to an open repair with a very low recurrence rate. This is called a urethroplasty.
When a stricture is first identified, it is commonly treated endoscopically (through a camera scope). We can use an assortment of devices such as a laser, cautery, balloon, etc. The recurrence rate for strictures is quite high. We now have good evidence to first try an endoscopic repair but if that fails to then consider moving on to an open repair with a very low recurrence rate. This is called a urethroplasty.
Urethroplasty
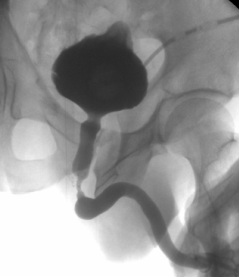
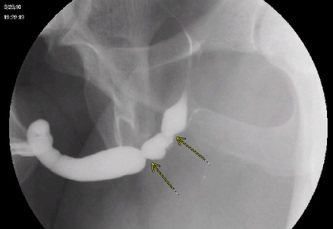
For large or recurrent urethral strictures, the "gold standard" of treatment with the lowest recurrence rates is an elegant surgical procedure called a urethroplasty. If the scarred tissue is quite small, simple excision of the diseased tissue is all that may be needed. For longer areas, like the one depicted in the picture, we would typically perform a graft procedure using buccal mucosa (inner cheek tissue). This is a very effective procedure that involves the Otolaryngologist obtaining the graft tissue from the cheek and the Urologist placing it to the affected and scarred urethra. Stricture recurrence rates are much lower and the results have excellent long term durability.
